
Antiviral Activity of Contemporary Contact Lens Care Solutions against Two Human Seasonal Coronavirus Strains


 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Contact Lens Care Products
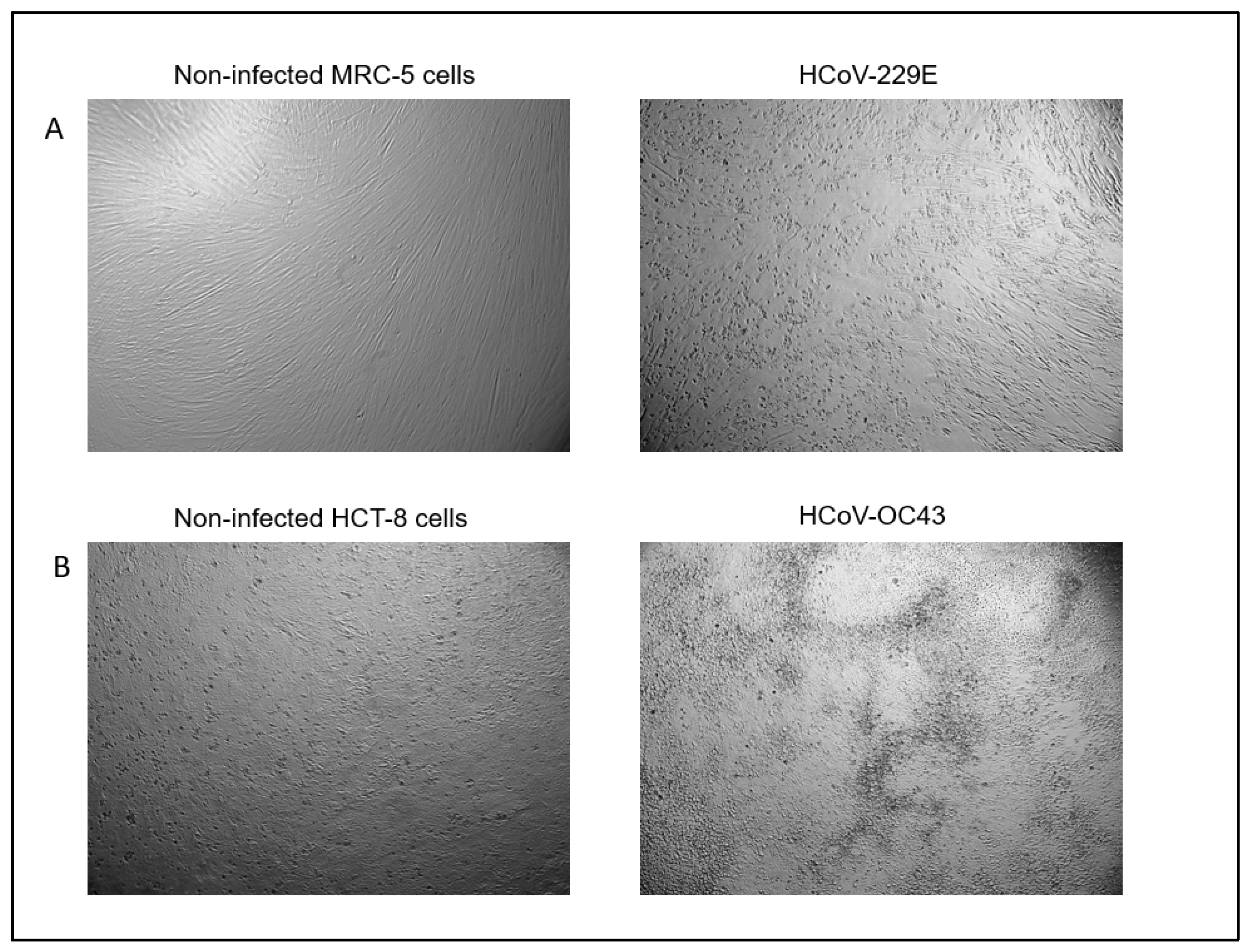
4.2. Virus and Cell Lines
4.3. Quantitative Suspension Test and Virus Titration
4.4. Controls
4.4.1. Cytotoxicity Control
4.4.2. Neutralization Control
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Peng, M.; Dai, J.; Sugali, C.K.; Rayana, N.P.; Mao, W. The Role of the Ocular Tissue in SARS-CoV-2 Transmission. Clin. Ophthalmol. 2020, 14, 3017–3024. [Google Scholar] [CrossRef] [PubMed]
- Ocansey, S.; Abu, E.K.; Abraham, C.H.; Owusu-Ansah, A.; Boadi-Kusi, S.B.; Ilechie, A.A.; Acheampong, D.O. Ocular Symptoms of SARS-CoV-2: Indication of Possible Ocular Transmission or Viral Shedding. Ocul. Immunol. Inflamm. 2020, 28, 1269–1279. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, X.; Chen, L.; Deng, C.; Zou, X.; Liu, W.; Yu, H.; Chen, C.; Sun, X. The evidence of SARS-CoV-2 infection on ocular surface. Ocul. Surf. 2020, 18, 360–362. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.-B.; Wang, Y.-Y.; Liu, G.-H.; Liu, Z. Role of the Eye in Transmitting Human Coronavirus: What We Know and What We Do Not Know. Front. Public Health 2020, 8, 155. [Google Scholar] [CrossRef] [Green Version]
- Qu, J.Y.; Xie, H.T.; Zhang, M.C. Evidence of SARS-CoV-2 Transmission Through the Ocular Route. Clin. Ophthalmol. 2021, 15, 687–696. [Google Scholar] [CrossRef]
- Barnett, B.P.; Wahlin, K.; Krawczyk, M.; Spencer, D.; Welsbie, D.; Afshari, N.; Chao, D. Potential of Ocular Transmission of SARS-CoV-2: A Review. Vision 2020, 4, 40. [Google Scholar] [CrossRef]
- Hui, K.P.; Cheung, M.C.; Perera, R.A.; Ng, K.C.; Bui, C.H.; Ho, J.C.; Ng, M.M.T.; Kuok, D.I.T.; Shih, K.C.; Tsao, S.-W.; et al. Tropism, replication competence, and innate immune responses of the coronavirus SARS-CoV-2 in human respiratory tract and conjunctiva: An analysis in ex-vivo and in-vitro cultures. Lancet Respir. Med. 2020, 8, 687–695. [Google Scholar] [CrossRef]
- Zhou, L.; Xu, Z.; Castiglione, G.M.; Soiberman, U.S.; Eberhart, C.G.; Duh, E.J. ACE2 and TMPRSS2 are expressed on the human ocular surface, suggesting susceptibility to SARS-CoV-2 infection. Ocul. Surf. 2020, 18, 537–544. [Google Scholar] [CrossRef]
- Grajewski, R.S.; Rokohl, A.C.; Becker, M.; Dewald, F.; Lehmann, C.; Fätkenheuer, G.; Cursiefen, C.; Klein, F.; Heindl, L.M. A missing link between SARS-CoV-2 and the eye?: ACE2 expression on the ocular surface. J. Med. Virol. 2021, 93, 78–79. [Google Scholar] [CrossRef]
- Deng, W.; Bao, L.; Gao, H.; Xiang, Z.; Qu, Y.; Song, Z.; Gong, S.; Liu, J.; Liu, J.; Yu, P.; et al. Ocular conjunctival inoculation of SARS-CoV-2 can cause mild COVID-19 in rhesus macaques. Nat. Commun. 2020, 11, 4400. [Google Scholar] [CrossRef]
- Akerman, D. Our greatest opportunity. Contact Lens Anterior Eye 2018, 41, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Walsh, K.; Willcox, M.; Morgan, P.; Nichols, J. The COVID-19 pandemic: Important considerations for contact lens practitioners. Contact Lens Anterior Eye 2020, 43, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Bajaj, A. Advances in self-assembled injectable hydrogels for cancer therapy. Biomater. Sci. 2020, 8, 2055–2073. [Google Scholar] [CrossRef] [PubMed]
- Kuc, C.J.; Lebow, K.A. Contact Lens Solutions and Contact Lens Discomfort: Examining the Correlations Between Solution Components, Keratitis, and Contact Lens Discomfort. Eye Contact Lens 2018, 44, 355–366. [Google Scholar] [CrossRef]
- Nichols, J.; Fisher, D. Contact lenses 2018. Contact Lens Spectr. 2019, 34, 18–23. [Google Scholar]
- Efron, N.; Nichols, J.J.; Woods, C.A.; Morgan, P.B. Trends in US Contact Lens Prescribing 2002 to 2014. Optom. Vis. Sci. 2015, 92, 758–767. [Google Scholar] [CrossRef] [Green Version]
- Nichols, J.J.; Chalmers, R.L.; Dumbleton, K.; Jones, L.; Lievens, C.W.; Merchea, M.M.; Szczotka-Flynn, L. The Case for Using Hydrogen Peroxide Contact Lens Care Solutions: A Review. Eye Contact Lens 2019, 45, 69–82. [Google Scholar] [CrossRef]
- Yamasaki, K.; Mizuno, Y.; Kitamura, Y.; Willcox, M. The Antimicrobial Activity of Multipurpose Disinfecting Solutions in the Presence of Different Organic Soils. Eye Contact Lens 2020, 46, 201–207. [Google Scholar] [CrossRef]
- Yamasaki, K.; Mizuno, Y.; Kitamura, Y.; McCanna, D.J.; Ngo, W.; Jones, L.W. The efficacy of povidone-iodine, hydrogen peroxide and a chemical multipurpose contact lens care system against Pseudomonas aeruginosa on various lens case surfaces. Contact Lens Anterior Eye 2021, 44, 18–23. [Google Scholar] [CrossRef]
- ISO/FDIS14729; Ophthalmic Optics—Contact Lens Care Products—Microbiological Requirements and Test Methods for Products and Regimens for Hygienic Management of Contact Lenses. International Organization for Standardization: Geneva, Switzerland, 2001.
- Schirtzinger, E.E.; Kim, Y.; Davis, A.S. Improving human coronavirus OC43 (HCoV-OC43) research comparability in studies using HCoV-OC43 as a surrogate for SARS-CoV-2. J. Virol. Methods 2022, 299, 114317. [Google Scholar] [CrossRef]
- Brüssow, H.; Brüssow, L. Clinical evidence that the pandemic from 1889 to 1891 commonly called the Russian flu might have been an earlier coronavirus pandemic. Microb. Biotechnol. 2021, 14, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Berche, P. The enigma of the 1889 Russian flu pandemic: A coronavirus? Presse Médicale 2022, 51, 104111. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 2249. [Google Scholar] [CrossRef] [PubMed]
- Cueno, M.E.; Imai, K. Structural Comparison of the SARS CoV 2 Spike Protein Relative to Other Human-Infecting Corona-viruses. Front. Med. 2020, 7, 594439. [Google Scholar] [CrossRef]
- Malik, Y.A. Properties of Coronavirus and SARS-CoV-2. Malays. J. Pathol. 2020, 42, 3–11. [Google Scholar]
- Enwemeka, C.S.; Bumah, V.V.; Mokili, J.L. Pulsed blue light inactivates two strains of human coronavirus. J. Photochem. Photobiol. B Biol. 2021, 222, 112282. [Google Scholar] [CrossRef]
- Mei, M.; Tan, X. Current Strategies of Antiviral Drug Discovery for COVID-19. Front. Mol. Biosci. 2021, 8, 671263. [Google Scholar] [CrossRef]
- Yasir, M.; Vijay, A.K.; Willcox, M. Antiviral effect of multipurpose contact lens disinfecting solutions against coronavirus. Contact Lens Anterior Eye 2021, 101513. [Google Scholar] [CrossRef]
- O’Donnell, V.B.; Thomas, D.; Stanton, R.; Maillard, J.Y.; Murphy, R.C.; Jones, S.A.; Humphreys, I.; Wakelam, M.J.O.; Fegan, C.; Wise, M.P.; et al. Potential Role of Oral Rinses Targeting the Viral Lipid Envelope in SARS-CoV-2 Infection. Function 2020, 1, zqaa002. [Google Scholar] [CrossRef]
- ASTM E1052-20; Standard Practice to Assess the Activity of Microbicides against Viruses in Suspension. ASTM International: West Conshohocken, PA, USA, 2020. Available online: https://www.astm.org/Standards/E1052.htm (accessed on 13 April 2022).
- Heaselgrave, W.; Lonnen, J.; Kilvington, S.; Santodomingo-Rubido, J.; Mori, O. The Disinfection Efficacy of MeniCare Soft Multipurpose Solution Against Acanthamoeba and Viruses Using Stand-Alone Biocidal and Regimen Testing. Eye Contact Lens 2010, 36, 90–95. [Google Scholar] [CrossRef]
- Kowalski, R.P.; Sundar-Raj, C.; Romanowski, E.G.; Gordon, Y. The disinfection of contact lenses contaminated with adenovirus. Am. J. Ophthalmol. 2001, 132, 777–779. [Google Scholar] [CrossRef]
- Wilson, L.A.; Sawant, A.D.; Ahearn, D.G. Comparative Efficacies of Soft Contact Lens Disinfectant Solutions Against Microbial Films in Lens Cases. Arch. Ophthalmol. 1991, 109, 1155–1157. [Google Scholar] [CrossRef] [PubMed]
- Lowe, R.; Vallas, V.; Brennan, N.A. Comparative efficacy of contact lens disinfection solutions. CLAO J. 1992, 18, 34–40. [Google Scholar]
- Mowrey-Mckee, M.; George, M. Contact Lens Solution Efficacy Against Acanthamoeba castellani. Eye Contact Lens 2007, 33, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Johnston, S.P.; Sriram, R.; Qvarnstrom, Y.; Roy, S.; Verani, J.; Yoder, J.; Lorick, S.; Roberts, J.; Beach, M.J.; Visvesvara, G. Resistance of Acanthamoeba Cysts to Disinfection in Multiple Contact Lens Solutions. J. Clin. Microbiol. 2009, 47, 2040–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildebrandt, C.; Wagner, D.; Kohlmann, T.; Kramer, A. In-vitro analysis of the microbicidal activity of 6 contact lens care solutions. BMC Infect Dis. 2012, 12, 241. [Google Scholar] [CrossRef] [Green Version]
- Retuerto, M.A.; Szczotka-Flynn, L.; Ho, D.; Mukherjee, P.; Ghannoum, M.A. Efficacy of Care Solutions Against Contact Lens-Associated Fusarium Biofilms. Optom. Vis. Sci. 2012, 89, 382–391. [Google Scholar] [CrossRef]
- Kilvington, S.; Winterton, L. Fibrous Catalyst–Enhanced Acanthamoeba Disinfection by Hydrogen Peroxide. Optom. Vis. Sci. 2017, 94, 1022–1028. [Google Scholar] [CrossRef]
- Szczotka-Flynn, L.B.; Imamura, Y.; Chandra, J.; Yu, C.; Mukherjee, P.K.; Pearlman, E.; Ghannoum, M.A. Increased Resistance of Contact Lens-Related Bacterial Biofilms to Antimicrobial Activity of Soft Contact Lens Care Solutions. Cornea 2009, 28, 918–926. [Google Scholar] [CrossRef] [Green Version]
- Russell, A.D. Similarities and differences in the responses of microorganisms to biocides. J. Antimicrob. Chemother. 2003, 52, 750–763. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.A.; Del Prete, A.; Lazzarino, A.I. Hydrogen peroxide and viral infections: A literature review with research hypothesis definition in relation to the current covid-19 pandemic. Med. Hypotheses 2020, 144, 109910. [Google Scholar] [CrossRef] [PubMed]
- Meyers, C.; Robison, R.; Milici, J.; Alam, S.; Quillen, D.; Goldenberg, D.; Kass, R. Lowering the transmission and spread of human coronavirus. J. Med. Virol. 2021, 93, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Comparison of In Vitro Inactivation of SARS CoV-2 with Hydrogen Peroxide and Povidone-Iodine Oral Antiseptic Rinses. J. Prosthodont. 2020, 29, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, M.; Roy, D.; Purohit, P.; Goyal, M.; Setia, P. Viricidal treatments for prevention of coronavirus infection. Pathog. Glob. Health 2020, 114, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract Pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kariwa, H.; Fujii, N.; Takashima, I. Inactivation of SARS Coronavirus by Means of Povidone-Iodine, Physical Conditions and Chemical Reagents. Dermatology 2006, 212, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Rapid In-Vitro Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Using Povidone-Iodine Oral Antiseptic Rinse. J. Prosthodont. 2020, 29, 529–533. [Google Scholar] [CrossRef]
- Anderson, D.E.; Sivalingam, V.; Kang, A.E.Z.; Ananthanarayanan, A.; Arumugam, H.; Jenkins, T.M.; Hadjiat, Y.; Eggers, M. Povidone-Iodine Demonstrates Rapid In Vitro Virucidal Activity Against SARS-CoV-2, The Virus Causing COVID-19 Disease. Infect. Dis. Ther. 2020, 9, 669–675. [Google Scholar] [CrossRef]
- Frank, S.; Brown, S.M.; Capriotti, J.A.; Westover, J.B.; Pelletier, J.S.; Tessema, B. In Vitro Efficacy of a Povidone-Iodine Nasal Antiseptic for Rapid Inactivation of SARS-CoV-2. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 1054–1058. [Google Scholar] [CrossRef]
- Kilvington, S. Antimicrobial efficacy of a povidone iodine (PI) and a one-step hydrogen peroxide contact lens disinfection system. Contact Lens Anterior Eye 2004, 27, 209–212. [Google Scholar] [CrossRef]
- Reed, L.J.; Muench, H. A simple method of estimating fifty per cent endpoints. Am. J. Epidemiol. 1938, 27, 493–497. [Google Scholar] [CrossRef]
- Blodgett, R. Most Probable Number from Serial Dilutions. FDA. 2020. Available online: https://www.fda.gov/food/laboratory-methods-food/bam-appendix-2-most-probable-number-serial-dilutions (accessed on 13 April 2022).
- Comité Européen de Normalisation. EN 14476: Chemical Disinfectants and Antiseptics. Virucidal Quantitative Suspension Test for Chemical Disinfectants and Antiseptics Used in Human Medicine. Test Method and Requirements [Phase 2, Step 1]. 2015. Available online: https://standards.iteh.ai/catalog/standards/cen/5e78911a-aedf-4456-90b7-39e1649f8acf/en-14476-2013a1-2015 (accessed on 13 April 2022).
- Butcko, V.; McMahon, T.T.; Joslin, C.E.; Jones, L. Microbial Keratitis and the Role of Rub and Rinsing. Eye Contact Lens 2007, 33, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Bandara, M.B.; Vijay, A.K.; Masoudi, S.; Wu, D.; Willcox, M. Importance of Rub and Rinse in Use of Multipurpose Contact Lens Solution. Optom. Vis. Sci. 2011, 88, 967–972. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 1% Test | 10% Test | |||
|---|---|---|---|---|
| HCoV-229E | HCoV-OC43 | HCoV-229E | HCoV-OC43 | |
| Biotrue | 0.04 ± 0.08 | 0.01 ± 0.09 | 0.12 ± 0.12 | 0.09 ± 0.04 |
| Boston Simplus | 0.12 ± 0.06 | 0.05 ± 0.08 | 0.12 ± 0.02 | 0.09 ± 0.04 |
| OPTI-FREE Puremoist | 0.04 ± 0.06 | 0.07 ± 0.09 | 0.10 ± 0.10 | 0.04 ± 0.00 |
| Clear Care | 0.02 ± 0.05 | 0.05 ± 0.08 | 0.08 ± 0.04 | 0.09 ± 0.04 |
| cleadew | 0.01 ± 0.04 | 0.12 ± 0.13 | 0.08 ± 0.07 | 0.09 ± 0.04 |
| cleadew GP | 0.10 ± 0.04 | 0.16 ± 0.06 | 0.03 ± 0.03 | 0.17 ± 0.04 |
| 1% Test | 10% Test | |||||||
|---|---|---|---|---|---|---|---|---|
| 4 h | p-Value * | 6 h | p-Value * | 4 h | p-Value * | 6 h | p-Value * | |
| Biotrue | 0.17 ± 0.10 | >0.99 | 0.10 ± 0.07 | 0.27 | 0.09 ± 0.07 | 0.9868 | 0.12 ± 0.13 | 0.9981 |
| Boston Simplus | 0.34 ± 0.11 | 0.95 | 0.57 ± 0.08 | <0.01 | 0.20 ± 0.06 | 0.6371 | 0.16 ± 0.09 | 0.9894 |
| OPTI-FREE Puremoist | 0.08 ± 0.12 | >0.99 | 0.25 ± 0.03 | <0.01 | 0.19 ± 0.07 | 0.6887 | 0.36 ± 0.09 | 0.6705 |
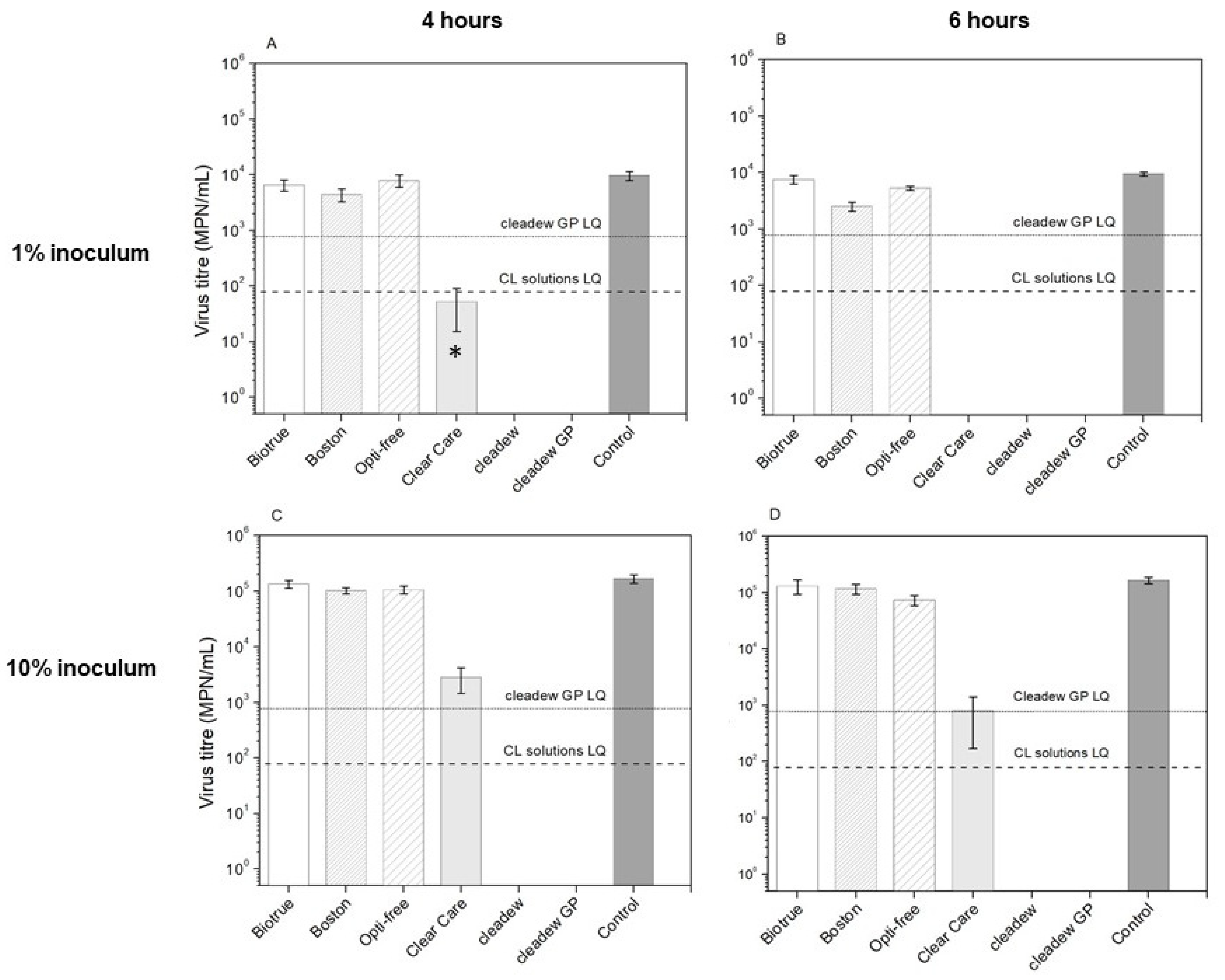
| Clear Care | 1.90 ± 0.09 | <0.01 | >2.08 | <0.01 | 1.84 ± 0.29 | <0.0001 | 2.57 ± 0.55 | <0.0001 |
| cleadew | >2.09 | <0.01 | >2.08 | <0.01 | >3.32 | <0.0001 | >3.32 | <0.0001 |
| cleadew GP | >1.09 | <0.01 | >1.08 | <0.01 | >2.32 | <0.0001 | >2.32 | <0.0001 |
| 1% Test | 10% Test | |||||||
|---|---|---|---|---|---|---|---|---|
| 4 h | p-Value * | 6 h | p-Value * | 4 h | p-Value * | 6 h | p-Value * | |
| Biotrue | 0.03 ± 0.09 | >0.99 | 0.04 ± 0.12 | 0.99 | 0.04 ± 0.01 | >0.9999 | 0.08 ± 0.06 | 0.7541 |
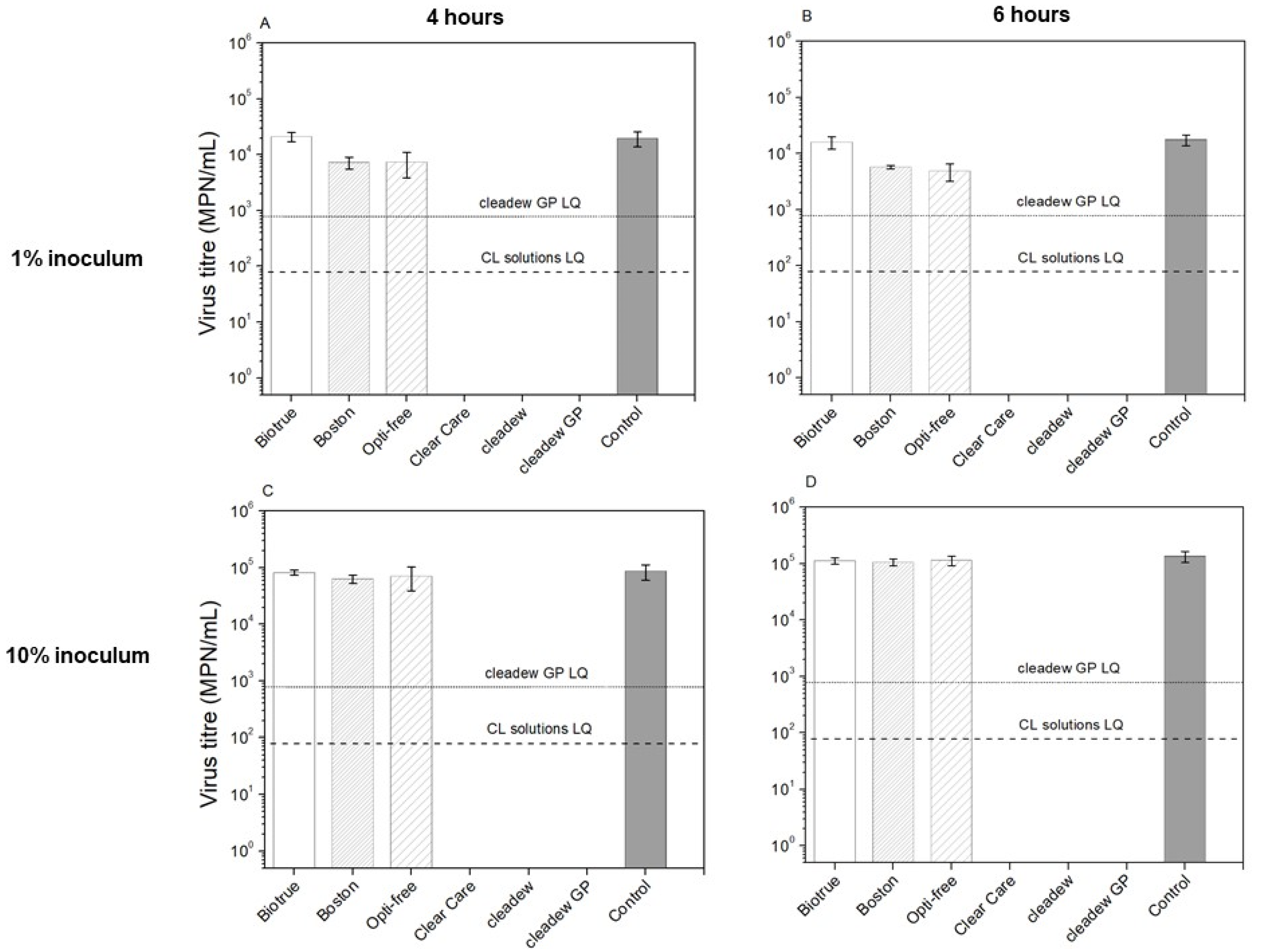
| Boston Simplus | 0.38 ± 0.10 | <0.01 | 0.53 ± 0.04 | <0.01 | 0.12 ± 0.07 | 0.8557 | 0.10 ± 0.06 | 0.9989 |
| OPTI-FREE Puremoist | 0.43 ± 0.19 | 0.01 | 0.56 ± 0.16 | <0.01 | 0.20 ± 0.05 | 0.9097 | 0.08 ± 0.08 | 0.8145 |
| Clear Care | >2.40 | <0.01 | >2.35 | <0.01 | >3.02 | <0.0001 | >3.23 | <0.0001 |
| cleadew | >2.40 | <0.01 | >2.35 | <0.01 | >3.02 | <0.0001 | >3.23 | <0.0001 |
| cleadew GP | >1.40 | <0.01 | >1.35 | <0.01 | >2.02 | <0.0001 | >2.23 | <0.0001 |
| Contact Lens Care Product | Manufacturer | Disinfectant Agents | Minimum Disinfection Time (h) |
|---|---|---|---|
| Biotrue | Bausch & Lomb, Rochester, NY, USA | Polyaminopropyl biguanide 0.00013% and polyquaternium 0.0001% | 4 |
| Boston Simplus | Bausch & Lomb, Rochester, NY, USA | 0.003% chlorhexidine gluconate and 0.0005% polyaminopropyl biguanide | 4 |
| OPTI-FREE Puremoist | Alcon, Fort Worth, TX, USA | Polyquad (Polyquaternium-1) 0.001% and Aldox (Myristamidopropyl Dimethylamine) | 6 |
| Clear Care | Alcon, Fort Worth, TX, USA | 3% hydrogen peroxide | 6 |
| cleadew | Ophtecs, Kobe, Japan | 0.05% Povidone-iodine | 4 |
| cleadew GP | Ophtecs, Kobe, Japan | 0.05% Povidone-iodine | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lourenco Nogueira, C.; Boegel, S.J.; Shukla, M.; Ngo, W.; Jones, L.; Aucoin, M.G. Antiviral Activity of Contemporary Contact Lens Care Solutions against Two Human Seasonal Coronavirus Strains. Pathogens 2022, 11, 472. https://doi.org/10.3390/pathogens11040472
Lourenco Nogueira C, Boegel SJ, Shukla M, Ngo W, Jones L, Aucoin MG. Antiviral Activity of Contemporary Contact Lens Care Solutions against Two Human Seasonal Coronavirus Strains. Pathogens. 2022; 11(4):472. https://doi.org/10.3390/pathogens11040472
Chicago/Turabian StyleLourenco Nogueira, Christiane, Scott Joseph Boegel, Manish Shukla, William Ngo, Lyndon Jones, and Marc G. Aucoin. 2022. "Antiviral Activity of Contemporary Contact Lens Care Solutions against Two Human Seasonal Coronavirus Strains" Pathogens 11, no. 4: 472. https://doi.org/10.3390/pathogens11040472